


































































QUICK SUMMARY
When enterprise hospitals roll out virtual care, the debate is always “buy vs. build.” Do you license a white-label telehealth platform for speed, or invest in custom development for ultimate control?
This guide bypasses biased marketing to reveal the actual engineering reality. We break down the underlying WebRTC telecom infrastructure, 5-year TCO, FHIR integration limits, and why the “Hybrid Model” may be the best choice for you.
Your board wants a fully integrated virtual care platform, and they want it launched by next quarter.
If you start researching your options, you will immediately hit a wall of biased vendor marketing. White-label providers will tell you that building custom software is a multi-million-dollar black hole that will take years. Custom development agencies will counter by saying white-label platforms are rigid, insecure rentals that will inevitably ruin your patient experience.
Neither side is telling you the whole truth because both have a product to sell you.
As telecom engineers who actually build the underlying WebRTC, SIP, and Session Border Controller (SBC) infrastructure that makes video conferencing in medicine possible, we don’t have a horse in this race. We don’t care if you rent the frontend or code it from scratch. We only care that the underlying architecture holds up when a patient is in a crisis and network latency spikes.
So, let’s look at the actual facts, the compliance realities, and the hidden infrastructure requirements of custom vs. white-label telehealth.
What is Custom Telehealth Platform Development?
Custom telehealth platform development means building your own proprietary virtual care software from scratch. You own the source code, you control the underlying media routing (WebRTC/SIP), you host the databases, and you dictate every single pixel of the user experience.
- Total architecture control: You decide exactly how audio and video packets are routed and encrypted.
- Deep EHR write-back: Ability to build bidirectional SMART on FHIR integrations tailored to your specific clinical workflows.
- No per-user licensing: You pay for your own cloud compute, meaning scaling from 100 to 10,000 doctors doesn’t exponentially inflate your software bills.
- Custom clinical tools: Integration with specific Bluetooth medical devices (like remote stethoscopes or IoT blood pressure cuffs) that off-the-shelf platforms don’t support.
Custom vs. White-Label Telehealth Platform
Before we look at the architecture, let’s clearly define the two ends of the spectrum to see what you are actually buying.
The White-Label Telehealth Platform
A white-label telehealth platform is a pre-built, fully functional software application created by a third-party vendor. You pay a licensing fee (usually per provider or per consultation) to use their cloud infrastructure, add your hospital’s logo and colors on the interface, and push it live to your patients.
It is the fastest path to market. You can launch a branded virtual clinic in 4 to 8 weeks. The vendor handles the server hosting, basic bug fixes, and feature updates. However, your differentiation is practically zero, your margins shrink as you scale, and you are entirely at the mercy of the vendor’s product roadmap.
Custom Telehealth Platform Development
It is exactly what it sounds like: building your proprietary virtual care software from the ground up. You own the source code, you control the media routing, you host the databases in your own cloud environment, and you dictate every single pixel of the user experience.
It is the path of maximum control and maximum initial friction. It requires a heavy upfront capital expenditure and a few months of development. However, once built, you pay zero per-user licensing fees, meaning your operating costs per consultation plummet as your patient volume scales. You can also build highly specific clinical workflows that off-the-shelf software simply cannot support.
Custom vs. White-Label Telehealth: The 5-Year TCO Comparison
| White-Label Platform | Custom Telehealth Platform | |
| Time to Market | 4 to 8 Weeks | 6 to 9 Months |
| Year 3-5 Operating Costs | Very High (Scaling per-user/per-minute fees) | Low (Only paying for raw cloud compute/bandwidth) |
| EHR Integration Depth | Shallow (Basic HL7 demographic pulls) | Deep (Bidirectional SMART on FHIR) |
| UI/UX Control | Limited (Colors, logos, basic layouts) | Absolute (Pixel-perfect clinical workflows) |
Want a virtual care platform that actually scales with your hospital?
How to Know You Have Outgrown Your White-Label Vendor?
Enterprises rarely start with a massive custom build. They usually launch with a white-label telehealth platform to test patient demand and secure quick wins. But considering 80% of consumers have now used telemedicine in their lifetime, that patient demand scales faster than ever, and eventually, you hit a ceiling.
Here are the signals that tell you it is time to migrate away from your vendor and build custom:
- The Margin Squeeze: Paying that big number was fine when you had 50 doctors. Now you have just acquired a clinic network and have 2,000 providers. The compounding licensing fees suddenly make owning your own cloud infrastructure significantly cheaper.
- The “Roadmap” Delays: Your clinical team needs a specific workflow, like routing a patient to a billing specialist immediately after a physician ends the call, or integrating a Bluetooth remote stethoscope. The vendor says, “We’ll add it to our roadmap for Q4 next year.” You are stuck waiting on someone else’s priorities.
- Trapped Data: You want to run advanced machine learning analytics on your patient interactions to predict readmission rates. But the vendor locks your raw database behind their proprietary API limits, preventing you from freely querying your own data.
The Hybrid Approach to Telehealth
For enterprise healthcare, the hybrid model isn’t just one of the options; it is becoming the default standard.
Most enterprises realize that the choice isn’t purely binary. You don’t have to code a video codec from scratch, but you also shouldn’t rent your entire clinical workflow forever.
The hybrid model allows you to license a CPaaS (Communications Platform as a Service) API or a headless white-label video engine while your developers build a highly customized patient app around it. You get the speed of a pre-built video backend with the workflow control of a custom frontend.
Later, if the vendor’s API gets too expensive at scale, you can swap out their video engine for your own open-source WebRTC media servers (like FreeSWITCH or Kamailio). Because you own the frontend app, you can change the backend plumbing without the doctors or patients ever noticing a disruption in service.
Ecosmob Expert Tip
If your custom telehealth app needs to transfer a patient from a virtual triage nurse to an on-call doctor’s actual cell phone, you are crossing from WebRTC into the public telephone network (PSTN). Many platforms struggle with this handoff. Ensure your Session Border Controller (SBC) is properly configured to handle seamless SIP REFER messages so the media stream doesn’t drop during that warm transfer to the mobile network.
The Telehealth Telecom Infrastructure
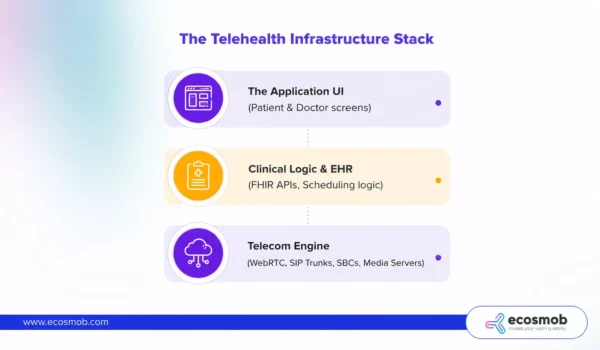
Whether you buy or build, your platform sits on top of Real-Time Communications (RTC) infrastructure. It is not just a standard web app; it is a live telecom engine.
- WebRTC: This is the open-source protocol that allows browsers and mobile apps to stream high-definition video and audio without requiring the patient to download a clunky plugin.
- Signaling (SIP/WebSockets): Before the video starts, the devices need to find each other across the internet. SIP (Session Initiation Protocol) or WebSockets handle the “ringing,” the connection setup, and the call end.
- Media Servers (SFU/MCU): Peer-to-peer WebRTC works fine for a 1-on-1 call. But if a doctor brings a translator and a specialist into the session, peer-to-peer can crash the patient’s CPU. You need a Selective Forwarding Unit (SFU) or Multipoint Control Unit (MCU) in the cloud to manage and distribute those multiple video streams efficiently.
When you buy a white-label telehealth platform, the vendor manages this entire telecom stack. When you choose custom telehealth platform development, you have to architect and manage this WebRTC infrastructure yourself.
Step-by-Step Enterprise Telehealth Launch Guide
Existing telehealth launch guides on the internet are written for small, independent clinics. They tell you to “train your staff” and “check your webcam.”
Launching in an enterprise hospital network requires strict IT governance and hardcore telecom engineering. Whether you go white-label or custom, here is the actual step-by-step technical reality of rolling out virtual care:
Step 1: Audit the BAA Subprocessor Chains (HIPAA Technical Safeguards)
Do not just sign the vendor’s top-level BAA (Business Associate Agreement). You must legally map out their entire subprocessor chain. If the platform uses AWS for database hosting and Twilio for the video API, your HIPAA technical safeguards must cover data traversing those underlying third-party nodes. Couple this with strict SSO (Single Sign-On) tied to your hospital’s Active Directory, so access can be revoked instantly.
Step 2: Architect Multi-EHR & FHIR Write-Back
Move beyond basic flat-file integrations that just push a PDF summary at the end of a call. Before launching, engineer bidirectional SMART on FHIR integrations. This ensures the telehealth platform can pull patient context and write clinical notes back into discrete fields across Epic, Cerner, or even complex multi-EHR environments simultaneously.
Step 3: Auto-Scale the Media Layer (The WebRTC Bottleneck)
Video traffic will crush your infrastructure if you treat it like standard web traffic. If a flu outbreak hits and concurrent sessions spike 400%, a static server architecture will crash. You must configure dynamic auto-scaling for your Selective Forwarding Units (SFUs) across your distributed microservices architecture, ensuring your media layer automatically spins up new compute nodes before the video quality degrades.
Step 4: Engineer SIP Trunk Fallback
What happens if the patient’s home Wi-Fi drops mid-call? A dropped call is a clinical risk. Ensure your platform is integrated with your core telecom stack so it can automatically failover. If the WebRTC video stream experiences heavy packet loss, the system should use SIP trunking to seamlessly dial the patient’s cell phone over the PSTN without disconnecting the session.
Step 5: Implement Real-Time Telemetry and Observability
You cannot fix dropped calls if you cannot see the packet loss. Do not launch without piping your SIP signaling, WebRTC logs, and RTP jitter metrics into an observability platform like Prometheus or Datadog. Your NOC needs real-time dashboards to identify whether a dropped call was caused by a hospital firewall blocking UDP ports or just a patient’s bad cell service.
Step 6: Endpoint and Network Calibration
A browser-based platform might run flawlessly on a developer’s MacBook, but lag horribly on the locked-down, thin-client virtual machines your nurses actually use. You must calibrate the media servers and configure your hospital firewalls to ensure UDP/WebRTC traffic is prioritized, preventing video degradation on legacy hospital hardware.
The Integration Reality: Flat Files vs. FHIR Write-Back
The platform pulls the patient’s name and pushes a flat PDF summary into Epic or Cerner after the call. Doctors still have to keep two screens open.
Custom development allows for Bidirectional SMART on FHIR Integration. Your custom video player can be embedded directly inside the EHR hyperspace. As the doctor takes notes in your app, the data writes back to specific, discrete FHIR fields in the patient’s medical record in real-time, saving minutes of documentation per visit.
Need help mapping your FHIR integrations and WebRTC media infrastructure?
Who Owns the HIPAA Liability in a Telehealth Platform?
You do. Always.
There is a massive, dangerous misconception that buying a “HIPAA compliant white-label platform” magically shields your hospital from legal liability. It does not.
When you use a white-label platform, the vendor signs a Business Associate Agreement (BAA). They are legally responsible for encrypting the data at rest and in transit on their servers. But if one of your doctors leaves their laptop open in a coffee shop, or if your IT admin misconfigures the user access permissions and exposes patient records, the HIPAA fine hits your organization.
When you build a custom platform, you own the entire compliance chain. You must configure the AWS/Azure instances securely, ensure your databases are wiping temporary Protected Health Information (PHI) correctly, and write your own audit-logging microservices.
It requires more engineering overhead, but it gives your compliance and security officers 100% visibility into the data architecture, eliminating the black box risk of third-party vendors.
The custom vs. white-label telehealth debate is not actually about software; it is about your organization’s budget structure and internal engineering talent.
If you need to launch a virtual clinic before the end of the quarter and you can’t get a dedicated team of software and VoIP developers, a white-label solution is your safest, most logical bet for now.
But if telehealth is a core, permanent pillar of your hospital’s revenue model, renting your infrastructure is a long-term trap. By investing in custom telehealth platform development, you take complete control of your media paths, eliminate compounding licensing fees, and build clinical workflows that actually integrate seamlessly into your physicians’ daily lives.
Don’t know if you should buy, build, or go hybrid? Let our telecom architects audit your clinical requirements and help you map the right infrastructure!
FAQs
When is custom telehealth development actually justified for an enterprise?
Custom development is justified when telehealth is a core revenue driver, and you need absolute control over the clinical workflow. It makes sense when you require deep, bidirectional EHR integration (like Epic or Cerner), integration with specific medical IoT devices, or when white-label per-user licensing fees start exceeding the cost of running your own cloud servers.
Custom or white-label telehealth platform, which has a lower total cost of ownership (TCO) over a 5-year horizon?
For small clinics, white-label is cheaper. But for an enterprise scaling to thousands of providers and hundreds of thousands of minutes, a custom platform has a significantly lower 5-year TCO. White-label vendors charge compounding per-user or per-minute fees. A custom platform requires a heavy upfront investment, but operational costs drop dramatically since you only pay for raw cloud compute and bandwidth.
How deep can EHR integration go with a white-label platform?
White-label EHR integration is typically shallow. It usually involves basic HL7 demographic pulls (getting the patient's name) and pushing a flat PDF summary into the EHR after the call. It rarely supports bidirectional SMART on FHIR integrations, which are required if you want your doctors to document directly in discrete EHR fields while on a video call.
What signals tell us we have outgrown a white-label platform?
You have outgrown your white-label platform when your vendor's per-user licensing fees become your largest IT expense, when critical feature requests take over six months to get on the vendor's roadmap, or when the platform's closed APIs prevent you from running advanced data analytics on your own patient interactions.
How do I launch a white-label telehealth platform securely?
Launching securely requires more than just signing a contract. Enterprises must audit the vendor's subprocessor BAA chain, enforce Single Sign-On (SSO) tied to the hospital’s Active Directory for instant access revocation, and test the platform's video performance on the hospital's specific internal network and hardware devices to ensure stable WebRTC connectivity.




